by Mindy Fried | Jun 10, 2016 | aging, connections with people, engaged aging, family, feminism, gender, health care, House Un-American Activities Committee, making choices, resiliency, theatre, Uncategorized, work and family balance
In this interview, Gayle Sulik, Founder of the Breast Cancer Consortium and Co-Founder of Feminist Reflections, talks with Mindy about her new book, Caring for Red: A Daughter’s Memoir (Vanderbilt University Press, forthcoming, Summer, 2016).
 GAYLE: Mindy Fried, your new book Caring for Red tells a story of you and your sister taking care of your 97-old father in the last year of his life in an assisted living facility. Before we talk about your experience caring for your dad, Manny, tell me a little about him. Who was this colorful character? After all, he earned the nickname “Red.” Sounds fiery to me!
GAYLE: Mindy Fried, your new book Caring for Red tells a story of you and your sister taking care of your 97-old father in the last year of his life in an assisted living facility. Before we talk about your experience caring for your dad, Manny, tell me a little about him. Who was this colorful character? After all, he earned the nickname “Red.” Sounds fiery to me!
MINDY: My father was a person with many lives. As a young man, he was a labor organizer for the United Electrical Workers union where he organized factory workers. That was when industrial labor was still predominantly based in the US, and not in third world countries where labor is cheaper. At some point, he joined the Communist Party. I’m not sure how active he was or for how long, but certainly at that time, being considered a “Communist” was tantamount to being a terrorist in our current political climate. In1954, when I was around 4 years old, he was subpoenaed to testify in front of the House Un-American Activities Committee (HUAC), a very traumatic experience for him, and for my whole family. He was “blacklisted”, meaning that when he applied for jobs, he was turned away. Eventually, he was hired by a Canadian company where he sold life insurance for around 15 years. That’s the kind of work he did through much of my childhood. But he was also writing plays based on his experience as a labor organizer, and he returned to the theatre as an actor, something he had done years before. When I was a teenager in the 1960s, he was subpoenaed by HUAC again. That was tough, but times had changed quite a bit and the ramifications weren’t quite as dire as they were the first time around. He ended up going back to school when he was in his 50s. Really impressive, since he had only one year of college under his belt. He went straight from finishing an undergraduate degree to working on a Ph.D. in English. His final career was as an English professor at SUNY Buffalo State College. You might say that nothing kept this guy down. He was a great role model in that sense.
GAYLE: How did your family survive the impact of the McCarthy period?
MINDY: I grew up with two people who were angry with each other often, but it was quiet anger. That was hard. I was lucky to have a best friend who moved in down the street from me when I was 5 years old, and her family basically adopted me. She liked my house because it was quiet, and I liked hers because it was lively and warm and loving. She became my “non-bio” sister, as we say; we’re still close today. Her parents became surrogate parents, and I am ever-grateful for that. They were just very attentive; my parents were often distracted. It was great to have another family a few doors down the street. That was one way I coped. But as a family, we also believed that my father made the right choices, in how he challenged HUAC, and continued to stand up for his beliefs. Having a sense of doing the right thing goes a long way.
GAYLE: Another name associated with Manny Fried, is “Morrie.” Six years before your father died, he played the character MORRIE in a play called Tuesdays with Morrie. As the story goes, a University graduate visits his former mentor, a sociologist who is slowly dying of a progressive disease. You write that your father inhabited that role fully, and that it helped to bring you closer together. Tell me why.
Well first of all, it was a big deal to play Morrie, not only because it was a great opportunity for my father, but also because he got to perform at the Studio Arena Theater, which had blacklisted him for many years. For me, the other exciting thing about him getting this role was that Morrie was a sociologist in my own department at Brandeis University. I knew Morrie, and the moment that my dad got the part, I saw it as an opportunity for the two of us to connect around his preparation and performance. I introduced him to Gordie Fellman, one of Morrie’s closest friends and colleagues from Brandeis. And I introduced him to a couple of Buddhists and sociologists who called themselves “Monday’s with Morrie”, as opposed to Tuesdays with Morrie (upon which the book and play were based). We also watched the Frontline TV series that Ted Koppel produced about Morrie, where Koppel interviewed him over the period of time as he was dying of ALS. When my dad came to visit me, he would have these meetings, and he would run his lines with me, and he would practice a grapevine dance from the play in my narrow hallway. It was just this really sweet thing that we connected around, and then obviously I always went to see him when he acted, so it was great to see him in the play, and he really did a beautiful job. People are always kind of amazed when they see old people function in any way, but seeing him excel at inhabiting this character – I think it was a really powerful experience for the audience and he pulled it off; he did a great job.
GAYLE: In your book, you describe a father who was loving – someone you felt deeply close with – but also a man who was full of himself. Did you feel resentment about taking care of him in this last year of his life?
MINDY: Well I think that this a really important question because as adult children, many of us have mixed feelings about our parents. The answer is “no”, I didn’t resent him. But it took me many years to understand him, to find equal footing with him, to find my voice with him, since he was a forceful speaker, sometimes controlling, and sometimes discounting of opinions that differed from his. He once told me that if I wasn’t sure about something, just guess, and that 99% of the time I’d be right. I was in my 30s when he gave me this advice, and by then I had his “number” and realized that this was sort of ridiculous. But he actually believed he was right most of the time! That said, I had deep respect for him and for his values and choices in life. He centered my world, for many years. In “exchange theory”, as it applies to families and relationships, the notion is that parents care for their children in one period of time, and later in life, when elder parents need support, children care for their parents. When it came time to care for my father, I did it with all my heart.
GAYLE: How did the father-daughter relationship change as Manny aged?
MINDY: My father and I were very close. Like most people, he was a flawed human being. He made serious choices in his life that impacted our family. But I had a deep respect for him, and we had a lot in common politically. For me, being part of the Women’s Movement in the 70s helped me better understand that despite being a good guy who was committed to social justice, he was pretty “old school”. I got frustrated with what a poor listener he was, and how I often had to fight for “air time” in conversations with him. But I did learn how to argue and debate because of him. I believe he felt I could be anyone or anything I wanted to be. And while he wasn’t comfortable “having or expressing feelings”, he was emotionally raw much of his life. That was one effect of McCarthyism on his life, and I understood that about him. Over the years, I understood enough of who he was to accept his shortcomings and his vulnerabilities and to just kind of let it go and say, “ok, here’s this person in the last bit of his life,” and to really be as fully present for him without losing myself.
GAYLE: You chronicle in your book many attempts, successful and unsuccessful, to find a place for your father to live that would meet his growing care needs AND offer the kind of life that fulfilled him. This was not easy, and sometimes your father was less than helpful. Tell me what worked, and what didn’t?
MINDY: I think one thing that worked was that I put myself in his shoes. For example, when we went and visited this super groovy retirement community that was connected to a college and he said to me, “there is absolutely no way I am going to move in there”. I imagined myself living with people that we met with, and I thought “I couldn’t do that either, this would be kind of horrible”. Not that they were bad people; it just felt foreign. These weren’t people he would choose to be friends with. I think that probably the most important thing as somebody gets older is to respect where they’re coming from. And I think it’s important to start thinking about these issues early on because you know, if you are trying to make a decision when it’s dire, the whole process of decision making is much more rife with emotion. I believe that talking about these things before you are in a crisis really makes a huge difference. And that helped us a lot.
GAYLE: Your father lived in Assisted Living for the final year of his life. Am I correct?
MINDY: Even though the book uses a one-year time frame, it was actually a year and a half that my sister and I cared for our father. It worked really well, until it didn’t. We learned what assisted living was able to provide for him as well as its limitations. Ultimately, in the last few months, he needed round the clock care. But he was able to live and die in his small apartment in assisted living. As an ethnography, Caring for Red provides a real sense of life in assisted living, the norms and values that drive human interaction, the hierarchy of staff, and the structures that define the experience within this institutional form of care that aims to provide a home-like environment.
GAYLE: Can you describe what Assisted Living is?
MINDY: Well, people think of it as kind of a hybrid health and home service, but in fact it’s really just more home than health oriented. It’s a place to live; there are regular meals; there often are activities; and staff provide services to residents – up to a point. Some assisted living facilities have medical staff; others don’t. We chose a place that had some nursing care, including medical people who delivered medications, and there was actually a doctor, a geriatrician, who came by once a week. But we had to pay for medical care because it was beyond the basic services offered. We ended up supplementing even more services in order to avoid having to send him to a nursing home. But that’s a longer story…
GAYLE: You were also a long-distance caregiver. How did you manage your father’s care from afar?
MINDY: I was lucky that I had a sister to do this with, so between the two of us we shared the caregiving work. We visited every weekend; we talked on the phone all the time; and we were on the phone constantly with caregivers, as well as his friends to help arrange his social life.
GAYLE: What do you hope for your book? How do you hope people will be affected by reading it?
MINDY: I guess if nothing else, I’d like it to contribute to a more open conversation about the trials and tribulations of caregiving work. While Caring for Red includes references to scholarly work on caregiving, I will be lucky if people feel more of a heart connection to the issues, particularly those people who are caring for an elder parent. We all have a range of feelings towards the people who cared for us when we were young. It’s important to recognize that there are a lot of people who love their parents; there are some people who hate their parents; and there are some people who have mixed feelings about their parents. Taking care of them in those final throes of life is jarring; AND it’s an opportunity to reconcile unresolved feelings; it’s an opportunity to treat elder parents with dignity and to make that last piece of life worth living. It’s also something that we’re all going to face at some point so I think that how we care for our parents is also a role model for how the younger people around us can – and hopefully will – care for us.
There’s no ultimate how-to book on caring for our parents. We all learn by what we see around us. So I’d like a dialogue to be stimulated about these issues. Because it’s very hard work – unpaid caregiving labor – and people don’t talk about this shit because it’s like, ‘oh it’s too depressing’, but hey, it’s life! We’re all going to die, you know, and somebody’s hopefully going to take care of us, so let’s think about how we want that to look within families and within society.
I also hope that academics will use this book in classes on aging, on death and dying, and on anything related to the life course. Moreover, Caring for Red is an ethnography, “set” in assisted living, so I hope it will be used in methods classes. And finally, for those who take interest in the history of facism and particularly, in the McCarthy era, the book presents quite a story, which I believe we must not lose.
GAYLE: Thank you, Mindy Fried. The deeply moving and insightful memoir – “Caring for Red”- is available for pre-order on Amazon.com.


by Mindy Fried | Jan 18, 2016 | adventure, aging, first job out of college, lessons learned, looking back, mental health, psychiatric care, sense of purpose

In the car were three patients from Hutchings Psychiatric Center. I was the driver, and we were out for a ride. It was the dead of winter in Syracuse, New York, where 40 below zero was par for the course. It was a biting cold that proffered no forgiveness, where any small swath of skin exposed would burn with a painful sharpness. But inside the car it was warm and cozy. And while Syracuse was known as a city with the least amount of sun in the U.S., second only to Seattle, which at least was surrounded by mountains, today in Syracuse there was sun. Sun that streamed into the car, warming the skin and the soul, defying the brutal Siberian temperature just outside of this metal contraption…
It was a special day. I was 21 years old and working as a dance therapist at Hutchings. How anyone trusted me to drive three patients – all recently released from long-term inpatient care – is beyond me. But I was trusted, by staff and presumably by these three patients who huddled in my off-white Chevrolet, my first car, bequeathed to me by my parents in recognition of my new adult status as a college graduate with a job. The car was used, bought by my father from his buddy, Mike, an auto mechanic at the local gas station. Mike promised my father it was safe; he had never steered my father wrong.

When I first saw it, I felt embarrassed by how clean and big and white it was. In my demographic, it wasn’t cool, like a VW bus was cool, and I worried about looking like the middle-class kid that I was. But it was wheels, and “she” soon bore the moniker, “Little Motherfucker”, younger sister to my friend’s giant Plymouth Duster, “Big Motherfucker”. She was a solid car, good enough to drive back and forth from Syracuse to Buffalo, my hometown. And certainly good enough to take three psychiatric patients for a spin…
Two of my favorite patients were in the car, a very tall, broad man with a long scruffy beard, oversized black glasses and an oversized nautical hat, who we called the Captain. He spoke with a gruff voice in short fragmented sentences; he was a sweet man, not very coherent, but always kind. Then there was Ruth Beam, a diminutive woman, maybe 4’8” and constantly shuffling in place, thanks to her meds; I think thorazine was the drug of choice at the time. She had a small nose, close-set eyes and a mouth that seemed to turn inward, as if she wanted to fade away. Ruth was labeled schizophrenic, and after leaving the hospital, she had moved back into a trailer with her husband, who purportedly had had an affair with her sister when she was hospitalized. How anyone knew that is unclear because Ruth didn’t speak, at best muttering incomprehensible phrases that seemed to narrate her hallucinations.

But in this moment, zooming down a New York State highway, sitting in a toasty warm car with the sun streaming in, I believe we all felt a sense of calm. There was no other place to be but where we were. I drove for an hour on highway roads, and then followed a few small roads towards Onondaga Lake. And when we arrived, we sat quietly in the car, pausing for a moment, and then slowly opened the doors, bracing our bodies against the cold. As I recall, we walked only a few feet towards the water, standing in a line parallel to the car, no one in a hurry. We stared out at the lake, a chill entering our bodies, but we had nothing to prove. So quickly did we get back in the car that I barely recall looking at the cold, hard ice or feeling gentle snowflakes touch my nose, the only body part exposed.
Back in the car, I felt the sun’s warmth on my face and the heat blasting through the vents. As we drove back, I savored the moments and felt a sadness that I wasn’t sure I understood.
I lasted in this job for one year. I was in way over my head. My supervisor, a lovely psychiatric nurse who treated me like a grown-up, told me that I had talent in working with this “population”. When I told her I was leaving, she encouraged me to return when I was ready. All I could think of was that I needed to get out, and I never looked back.
What drew me to work with people with psychiatric problems, coming from a family that had its share, was the exact reason why I had to get out. I had saved up as much money as I could in this one year, and left for Europe where I roamed freely for eight months, until it hit me that I had lost my sense of purpose. And that was how I learned that that was what life was about, having a sense of purpose. In my mind’s eye, I can still see the Captain and Ruth, and other patients who were assigned to me. I shudder when I think about my utter incompetence, but I was young and learning, a process I’ve discovered continues throughout life. As I think back to that day in the car, I know that we all felt a sense of adventure, with the knowledge that in our own way, just for an afternoon, sitting in the car for an hour’s ride in one direction, and then back again, with a short respite in the biting cold, we were free.

by Mindy Fried | Sep 6, 2015 | aging, applied sociology, connections with people, engaged aging, gender, making choices, research, social science research, SWAN Study, women and health
 I sit opposite Lila [1], the 25-year-old research assistant, in a small room at a satellite office of Mass General Hospital. She is warm and professional, and we have already discovered that she went to college at the same university where I went to graduate school. She took classes with some of my favorite professors, and we may have been in the same room at one point, when I came back to give a talk on campus. This is a nice ice-breaker. But now, in this room, Lila is in the driver’s seat. She has just finished asking me a load of questions about my health, lifestyle, and social networks. I will be there a total of four hours by the time I complete the entire process, which includes a bone density scan and a few other tests they’ve added this year.
I sit opposite Lila [1], the 25-year-old research assistant, in a small room at a satellite office of Mass General Hospital. She is warm and professional, and we have already discovered that she went to college at the same university where I went to graduate school. She took classes with some of my favorite professors, and we may have been in the same room at one point, when I came back to give a talk on campus. This is a nice ice-breaker. But now, in this room, Lila is in the driver’s seat. She has just finished asking me a load of questions about my health, lifestyle, and social networks. I will be there a total of four hours by the time I complete the entire process, which includes a bone density scan and a few other tests they’ve added this year.
 In 1996, right after I completed my Ph.D. in Sociology, I was randomly selected as one of 3,302 women from diverse racial/ethnic backgrounds to participate in this mid-life women’s health study called SWAN – or Study of Women’s Health Across the Nation. The study is following women as we transition through menopause, to better understand the physical, biological, psychological and social changes we experience during this period. SWAN aims to help scientists, health care providers and women “learn how mid-life experiences affect health and quality of life during aging”. [2]
In 1996, right after I completed my Ph.D. in Sociology, I was randomly selected as one of 3,302 women from diverse racial/ethnic backgrounds to participate in this mid-life women’s health study called SWAN – or Study of Women’s Health Across the Nation. The study is following women as we transition through menopause, to better understand the physical, biological, psychological and social changes we experience during this period. SWAN aims to help scientists, health care providers and women “learn how mid-life experiences affect health and quality of life during aging”. [2]
SWAN participants or “subjects” were all between 42 and 52 years old “at baseline” – that, is, when the study began – and we represent seven cities around the country, including my own city of Boston.
When I got the call inviting me to join the SWAN study, I had just completed a lengthy project that involved a lot of interviewing. I welcomed the opportunity to answer someone else’s questions! It also felt great to be a part of important research that had the prospects of influencing medical science. But when I said “yes” to participating in SWAN nearly 20 years ago, I could not have predicted that I would be interviewed by at least 10 or more 20-something research assistants, most of them en route to medical school following this “real-life” experience.
Last year, there was a funding hiatus for the study. I was having a tough year myself and barely noticed that I hadn’t gotten my annual call to set up an appointment. Then a month ago, a letter arrived. SWAN was back in biz, and I’d be getting a call soon! I was thrilled that the study was re-funded in this era of budget cuts for basic science and social science research. I was also feeling grateful that my health was back on track. It struck me that SWAN gave me a regular opportunity to reflect on my life’s circumstances, and to think about how I’m handling growing older, even if it’s only because of a series of questions read to me by a young research assistant whom I’ve just met.
Lila was trained to draw blood, and as she jabs me with the needle, I think, wow, she’s pretty good. We continue to chat, as she measures my waist and hips, clocks how fast I can walk down the narrow hallway, and how long I can balance in a variety of different positions. I’m feeling pretty cocky, until we get to the cognitive test, which they instituted about four years ago. Even though I think my memory is pretty good, being quizzed by a millennial is unnerving. I tell Lila that this test makes me anxious, and she says “yeah, everyone hates it”. That’s only somewhat reassuring, but I appreciate her attempt to normalize my response. Once it’s over – after I spat back a series of numbers and letters in order, and re-told a story about three children in a burning house being saved by a brave fire fighter – I tell myself, “good enough”. That was something my father used to say in moments of stress.
The SWAN Study has taken care to ensure that we are a diverse sample of participants.
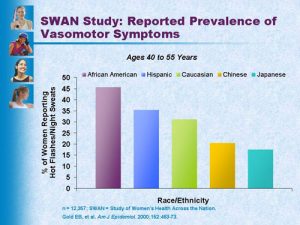
- Prevalence of hot flashes by race/ethnicity
In Boston, researchers over-sampled African-American women, meaning that the study has intentionally included a larger percentage of African-Americans than are represented in the general population. Other cities have ensured that the sample includes large numbers of Chinese, Japanese, and Hispanic women. This oversampling strategy allows researchers to investigate the influence of race and ethnicity on health outcomes of women as we age.
SWAN-affiliated researchers, Drs. Robin Green and Nanette Santoro, found that most symptoms of menopausal women varied by ethnicity. They write,
“Vasomotor symptoms were more prevalent in African-American and Hispanic women and were also more common in women with greater BMI, challenging the widely held belief that obesity is protective against vasomotor symptoms”.
They also found that vaginal dryness was present in 30-40 percent of SWAN participants at baseline, and was most prevalent in Hispanic women. But even among Hispanic women, “symptoms varied by country of origin”. The researchers conclude that “acculturation appears to play a complex role in menopausal symptomatology” and that “ethnicity should be taken into account when interpreting menopausal symptom presentation in women”.
By including an ethnically diverse sample, the SWAN Study is able to compare the experiences of women from varied backgrounds, which has pointed to important differences that should be of great benefit to health care practitioners. Moreover, SWAN researchers provide participants with information about our health, and flag issues we should explore further. For example, I discovered that I had high cholesterol, something that runs in my family. I’m now being monitored by a specialist, who asked me to take a very lose dose of a Statin. And overall, I’m more conscientious about my diet. The upshot is that my cholesterol levels are under control.
Gathering the SWANS…

- Jocelyn Elders, former U.S. Surgeon General
In the past couple of decades, the SWAN team held a number of gatherings to bring Boston SWAN “subjects” together. It’s awesome to be in a room with hundreds of women with one thing in common: we are mid-life women who have gone through menopause! What fun to talk about all the crap we are experiencing without feeling judged or worrying that we might be boring someone.
The first gathering I attended offered workshops where “experts” could answer our questions about sleep (like hot flashes keeping us awake) or provide us with alternatives to Hormone Replacement Therapy. One year, SWAN researchers organized an event that featured the brilliant and outspoken Jocelyn Elders, former U.S. Surgeon General who was a lightning rod for speaking her mind, in support of legalizing marijuana, the distribution of contraceptives in schools, and even suggesting that masturbation might be a means of preventing young people from engaging in riskier forms of sexual activity. Sitting in a diverse crowd of mid-life women and cheering for Elders, whom I have admired for years, was positively thrilling.
Lila tells me a little about this year’s gathering, which I unfortunately missed. I learn that one of the Boston-based Principal Investigators, Dr. Joel Finkelstein, is a serious art aficionado and at the last SWAN Study gathering, he showed a series of paintings by an older woman. His message was that we can continue to grow and be creative as we age. When the interview is complete, Lila hands me my gift. In past years, it has been a cup or a small tote bag, marked with the graceful SWAN logo. But this year, it’s a small box, the top graced with a floral design from this artist.

In the abstract of his 2014 application to the National Institutes of Health, Dr. Finkelstein concluded by saying, “SWAN will fill important gaps in understanding the impact of the menopausal transition and mid-life aging on women’s health and functioning in the postmenopausal years. Accordingly, it will provide useful information to guide clinical decisions in mid-life and beyond in women who have diverse life experiences and socioeconomic and racial/ethnic characteristics”.
I’m grateful to be a part of this longitudinal study, to know that the aggregate data being collected reflects a diverse population of women, and that we are collectively contributing to scientific knowledge that can improve the lives of women as we age.
Finally, here’s a great clip from Menopause, the Musical!, just for fun: https://www.youtube.com/watch?v=ndFBFXV3jjs
[1] Fictitious name
[2] The SWAN Study is co-sponsored by the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR), the National Institutes of Health (NIH), Office of Research on Women’s Health, and the National Center for Complementary and Alternative Medicine.
by Mindy Fried | Jul 4, 2015 | aging, connections with people, depression, engaged aging, exhaustion, gender, health, insomnia, resiliency, sleep, women and health, work culture
The men in my family were easy sleepers. It wasn’t uncommon to see my father and his six brothers lie down on the floor after a big meal and just nod out. Of course, that left my aunts to clean up, after they had also cooked the meal, and I bet they could have used a nap too. At the time, I figured that taking a post-meal snooze was the “way things were” for the men in the family. But gradually, as I developed a feminist consciousness, I resented these lazy guys. As my age gradually crept up to where theirs were back then, I have begun to appreciate their supreme capacity to sleep just about anywhere, anytime. My father was also one of those people who could nod out for five minutes – taking a so-called “power nap” – only to emerge refreshed and able to fully re-enter the conversation when he awoke.
Later, when he was in his 90s, he began to experience serious insomnia, lying awake for hours and hours throughout the night, going crazy with boredom and frustration. While I sympathized with his dilemma at the time, it wasn’t until I experienced my own sustained insomnia – after a back injury – that I understood how horrible it is to not be able to sleep night after night. I discovered that sleep deprivation steals one’s energy, one’s optimism, and sometimes even one’s sanity. With increasing lack of sleep, the exhaustion compounds and the world becomes slightly, if not majorly, off-kilter.

Insomnia is a lot of things, which includes having a hard time getting to sleep, as well as waking up early and having a difficult time getting back to sleep. Not surprisingly, it isn’t a contemporary phenomenon. No, we in the so-called modern world didn’t invent it. Insomnia goes way, way back. The term “insomnia” first appeared in 1623, and means “want of sleep”. One of the biggest causes of insomnia, stress, is something that people have been struggling with for eons. It’s just the nature of stress that looks slightly different these days, compared to a few centuries ago. But if you think about it, there are a lot of similarities.
We’re stressed because we work hard or we don’t have enough work. We’re stressed because we live in a violent world that is unpredictable. We’re stressed if we experience social isolation or prejudice. We’re stressed when we don’t have enough to eat, and don’t know where the next meal is coming from. We’re stressed because our jobs are too demanding or not challenging enough. We’re stressed because we worry about paying our bills. We’re stressed because we don’t feel loved enough, or because we have tension with our partners or our friends. One might call these universal problems, and these stressers will vary based on your economic situation as well as your race, gender and sexual identity. And maybe a few centuries ago, we might have also worried about predators or major diseases that wiped out entire swaths of people. All of these stressors can lead to loss of sleep.

A lot of famous people are recorded as having suffered from insomnia. Sir Isaac Newton suffered from depression and had difficulty sleeping. Winston Churchill had two beds because if he couldn’t sleep in one, he would try the other. Thomas Edison, like my father, was a cat-napper, because he couldn’t sleep at night. Some insomniacs turned to drugs. Marcel Proust and Marilyn Monroe took barbiturates to help them sleep. English writer, Evelyn Waugh, took bromides to induce sleep. As we know, Michael Jackson died because of a lethal cocktail of medications to help him sleep, including propofal, used for sedation before surgeries, lorazepam, used for anxiety, and a host of other meds, including midazolam, diazepam, lidocaine and ephedrine. He was obviously so desperate to sleep that he was willing to try them all.

Author and columnist Arianna Huffington calls insomnia a “feminist issue”, and has written columns in Huffington Post lamenting her lack of sleep from jet lag. Another Huff Post columnist, Dora Levy Mossanen, calls insomnia a “smart, devious virus that mutates and changes form every season like the flu virus. Except that this tricky bugger is tuned to our circadian rhythm and is able to change and disguise itself at whim to confuse the heck out of us”. Mossanen does all the “right things”: She doesn’t drink caffeine, goes to bed at a decent hour, drinks hot milk before bedtime, takes warm baths, reads non-stimulating books, listens to guided meditation on her i-pod, and imagines serene seashores. And yet she says, “I toss and turn at the beginning of the night, counting backwards and forwards so many times that if my mind was prone to mathematics, I’d have solved all the mathematical problems of the world by now”.
For the most part, my insomnia has cleared, but every so often it rears its ugly head. While in the midst of a minor insomniac “relapse”, I asked my friends and colleagues for their insomnia narratives. I wanted to know how long their insomnia lasted, why they thought they were struggling with sleep; what they did when they were awake; how it affected them the next day. I learned that the main causes of insomnia are:
* Anxiety, the everyday kind like preparing to teach a class, and larger anxieties, like worrying about keeping a job;
* Depression, which impedes relaxation necessary to fall and stay asleep;
* Medications, because some meds like decongestants and pain meds keep us awake. Antihistamines might initially make us groggy, but they can cause excess urination which gets us up a lot during the night;
* Alcohol, which may make you more relaxed, but prevents deeper stages of sleep and can cause you to wake up in the middle of the night;
* Chronic pain, which is distracting and worrisome and can lead to anxiety, which prevents sleep;
* Medical conditions, like arthritis, cancer, heart disease and Parkinson’s disease, which are linked with insomnia;
* Poor sleep habits, like weird sleep schedules, or an uncomfortable sleep environment;
* “Learned insomnia” – which is worrying too much about not being able to sleep, which makes it hard to get to sleep; and
* Eating too much before sleeping or eating the wrong snack, which can give you heartburn and make it uncomfortable to fall sleep.
In response to my call for insomnia stories, only women replied. I know that isn’t because men don’t experience insomnia; but perhaps men don’t want to reveal their sleeping problems publicly, even though I promised confidentiality. (It’s not too late, for my male readers!)
One woman said, “You do realize you’ve opened the floodgates, yes? Amazing topic. Of course, I’m too sleep-deprived and deep into end-of-semester madness to respond right now! Maybe during my next bout of insomnia (perhaps tonite). ;-)”
Here are a few responses from other insomniacs:
One woman says, “Funny you should ask, as I am suffering from insomnia just now, maybe a week long bout this time, but by far not the longest ever. I wake up about 4am and cannot fall back asleep if my life depended on it. Not sure why I have such a hard time staying asleep, maybe it’s hormonal (menopause) or maybe it’s all the craziness at the office (new department chair, no office support as the old secretary retired, research lagging, …). Often I am not the only one awake, as my spouse is also a stressed-out insomniac. I typically try to fall back asleep, but if it doesn’t happen, I get up and read in the living room until I feel exhausted from being up at 4 am. What sometimes works is counting backwards from 100 in another language. Needless to say, the next day I feel a bit out of it, but nothing like the “zombieness” I did when my child used to wake me up. I am not desperate yet, but may try to find my melatonin from the previous bout to get me back on track. Sometimes it works, sometimes it doesn’t”.
Another woman says, “My insomnia stories are boring. I get up and clean the house, read, catch up and/or get ahead on my work. That makes me feel like I am not wasting my time trying to fall asleep. Usually that day I am racing, energetic and feel good about all I have accomplished. By that night I am crashing and I pay the next day in bodily aches/pain. Not very exciting…”
Another says, “I have had quite a few episodes of insomnia. There were times when I would go days or even a week without adequate sleep. I would either fall asleep and then wake up in the middle of the night and not be able to go back to bed, or I would just simply stare at the ceiling until I finally fell asleep, only to wake up about every half an hour for the rest of the night. Either way, insomnia sucks! I eventually couldn’t take it any longer and sought medical help. Come to find out, I have general anxiety disorder and that was greatly affecting my sleep. Even now – I am on medication- I still have bouts of insomnia when I am highly stressed. My mind is constantly going, so when something important is coming up I find myself having trouble sleeping. In the middle of the night I have tried a number of things: read a book, go to the gym (thank you, 24 hour fitness), eat, watch TV, and try and go back to sleep. As a student, during the day I am pretty much reading, writing, researching, or preparing for a class I TA for.
“After a night of insomnia, I usually feel terrible the next day. Even if I am tired, I don’t try and nap because if I do, the likelihood of getting a good night’s sleep decreases. If I go a few days or even a week without sleep, my brain has pretty much checked out. I go through the motions but I don’t feel like I am really all there. Hopefully that makes sense. Insights? I would say that everyone is different and should try different things to help them sleep. I hate taking medicine, even when I am sick, so seeing a doctor was the last thing on my list. I tried doing yoga, eating better, not watching TV or reading at night…but nothing helped me. Being put on medication was a great relief because I sleep really well, for the most part”.
And finally, one of my neighbors says, “Sometimes I look out the window to see who else might be up in the neighborhood. I am tempted to text them or call and get together, maybe we should start an insomniac club”.
That sounds tempting… I suppose that one strategy I’m employing is writing this post. Maybe “outing myself” as an insomniac will help diffuse the potency of this insidious problem. If I were to characterize my current “brand” of insomnia, it’s “learned insomnia”, meaning that I begin to fall asleep and then just as I’m fading into a hazy fog, my brain says “you’re falling asleep”, at which point I’m awake! Luckily, the problem has lessened since I first put out the call for insomnia stories. May it fade away!
Tell me your insomnia story! What has helped you overcome your sleeplessness?
by Mindy Fried | Feb 1, 2015 | aging, health, Manny Fried, parenting, stress, support, value of caregiving work
My father’s hair had grown wild and unruly, and I told him, “You look like the mad Professor”, hoping for a smile from this working class guy from Buffalo turned local revolutionary hero. His strands of thin, white hair lingered in mid-air with nowhere to go, suspended in time and place, as his body recuperated from hip surgery that was probably a bad idea at age 94. Instead of feeling hopeful, he was despairing, wondering whether he had made the right decision, all the while trying to convince himself that he had. I couldn’t help but join him in this sentiment. I tried to be positive, reminding him that you can’t gauge improvement on a daily basis. It would take weeks, maybe months. But at his age, that’s playing with fire. Why the hell he insisted on having the surgery was beyond me. And why the hell his doctor didn’t say no just made me mad.
![]()
Over the years, I had become his make-shift hairdresser, a role that I relished. It was a way to connect with him in a contained window with a dollop of distance. For my atheist father, getting a haircut from me was a little like going to church, a solemn occasion filled with contemplation and calm. For me? I felt purposeful, able to help this man who had been such a stalwart support for so many years. The truth was that there was very little actual cutting of hair involved, but the ritual called for a slow pace and gentle hands. Using my scissors gingerly, I always started on the sides where the hairs were most prominent. The top hairs were next; they were sparse and the task of cutting was only a prelude to what would come later. I lingered at the back of his head because he knew it was almost over. And for the finale, I finished the job with an electronic razor to smooth it all out.
![]()
As I look back on this simple act of love, I relish in the peace I was able to bring to him. A firebrand in his day, he was losing steam, at times wondering if life was worth living. That was the hardest part for me. But this pure connection momentarily stripped away his cares and mine, and allowed us to be in the room together. When I stepped back to assess my work, I would always find wild hairs I missed. There is no perfection here. Only a work in progress. In the end, my father was quietly grateful. Not a man given to ‘thank you’s’, even in the best of times.
by Mindy Fried | Apr 20, 2014 | aging, connections with people, engaged aging, family, gender, making choices, retirement, social science research, women and work
re•tire [ri-tahyuh r]
1. to withdraw, or go away or apart, to a place of privacy, shelter, or seclusion: “He retired to his study”.
2. to fall back or retreat in an orderly fashion and according to plan, as from battle, an untenable position, danger, etc.
3. to withdraw or remove oneself: “After announcing the guests, the butler retired”.
4. to withdraw from office, business, or active life, usually because of age: to retire at the age of sixty.
5. retirement or withdrawal, as from worldly matters or the company of others.
One of my friends is passionate about Latin America and travels widely, monitoring elections and writing for an international journal. Her life-long “career” as an energy consultant is gradually shifting to her passionate “avocation”.
A family member who is a therapist decided to significantly pull back on her work hours, but then it didn’t “feel right”. Instead of leaving her practice, she decided to slow down the process, and continues to see clients. She is working fewer hours, spends more time with her children and grandchildren, and has increased her volunteer work.
Another friend had a decades-long successful career as a librarian. As her retirement approached, she was uncertain about what would come next, but stayed open to possibilities. She now works as a volunteer in a number of non-profit organizations, travels, reads, and has time to hang out with friends and former colleagues.
And me? I don’t plan to retire for a long time. First off, even though I’m technically approaching the typical “retirement age”, I like to work because I’d like to think that I’m contributing to making the world a slightly better place, at least in the small piece of the universe I inhabit. Maybe more basic is the fact that, like many people, I can’t afford to retire!
When it comes to major life changes, I like to be fully informed, so I decided to study “retirement narratives”. It’s an informal study that is personally driven by my desire to remain engaged in and satisfied with life when I stop working for pay someday (who knows which day). My study is a pre-emptive strike against loneliness and a concern that as I age, I will be on the periphery, no longer a contributor to the world, no longer a player in daily life…I know this can happen because I’ve seen it happen, and I bet you have too. My observations and intuition have been confirmed by reading a ton of books about aging, in preparation for an aging course I taught at Brandeis University, as well as following the substantial media coverage of issues of aging. My feeling was that my informal study would provide me with an opportunity to better understand this life changing event from a sociological perspective.

My role model for retirement was my father, who didn’t stop working in his job as an English professor until he was around 95 years old. I used to think that his formula – essentially, to never stop working – was how I wanted to live my life. I, too, imagined that I would basically work full-time until I dropped. But now I’m re-thinking my plans. And that’s where my research comes in. My study basically consists of informal “interviews” with friends who are reducing their paid work hours, as well as informal “chats” with acquaintances I run into in random places, like CVS, walking around Jamaica Pond, and on the street. For the people I know and with whom I have regular contact, I plan to follow them over a long period of time, meaning that I want to see what they do and how they adjust for as long as I know them, which could be until I or they die. With these friends, I hear the intimate details of their decision-making. Some of them had full-time jobs in organizations or institutions that provide incentives to retire, and some worried that they might lose their jobs past a certain age. Others work more autonomously as therapists or consultants.
 I want to understand how these friends feel about their paid job as they consider “winding down”: What do they consider will supplant the intense time and commitment they have made to this work? Do they have fears about retirement? Do they have passions they plan to pursue, and plans in place? Do they view retirement as an abyss or a welcome opportunity, neither or both? What will the transition period away from paid work be like? Do they just stop working for pay one day, or do they gradually decrease their hours, and increase the time they spend doing unpaid work or having fun! (imagine that!) How happy are they after retirement, which may include how active they are and how social they are? And lest we forget, how does their health – or the health of their partner – factor into the equation?
I want to understand how these friends feel about their paid job as they consider “winding down”: What do they consider will supplant the intense time and commitment they have made to this work? Do they have fears about retirement? Do they have passions they plan to pursue, and plans in place? Do they view retirement as an abyss or a welcome opportunity, neither or both? What will the transition period away from paid work be like? Do they just stop working for pay one day, or do they gradually decrease their hours, and increase the time they spend doing unpaid work or having fun! (imagine that!) How happy are they after retirement, which may include how active they are and how social they are? And lest we forget, how does their health – or the health of their partner – factor into the equation?
The research questions I employ with my “almost, kinda” friends have a one-two punch. We start by asking one another a few basic questions: “How are you?”, is the starter. Can’t get more basic than that! And then a probing question: “And what have you been up to?” Now this question also seems pretty basic but the reply reveals a lot through their words as well as their body language. If/when they say they’re retired – or just that they left their job of many years – my panoply of probes is unleashed and I ask, “Is it a good thing?” This is a general yes-no question, followed up by “How do you fill your days?” That’s the meat of what I’m looking for.

My informal study has no real parameters. My “sample” is fairly random; it’s not designed with any demographic in mind; I’ll talk to anyone. I’m not keeping track of how many people I’m interviewing, and I’m cool with going with the flow of the conversation, wherever it leads. I’m not discovering anything new, in a broader sense. There’s plenty of literature that argues for continued engagement in life, as one ages. Instead, my study is about getting at the particulars. What do people do as they’re considering retirement? Do they consciously prepare? Once they retire, what are they doing and how do they feel about it?
The issue of retirement has become even more salient because we are living longer. For example, in 2000, the life expectancy in the U.S. for women was 77.6, and for men it was 74.3. In 2010, those numbers had jumped to 79 and 76 respectively. It’s important to note that there is also a racial disparity, as reflected in 2010 figures, with white women projected to live until they are 81.3, and African-American women projected to live until they are 78. For men, the comparison between white and African-American men is 76.5 to 71.8, respectively.

Despite these gender and race disparities, an increase in longevity has resulted in a larger gap in time between official retirement and the point where people stop working for pay altogether. Dr. Mo Wang from the University of Maryland calls this period “post-retirement”, a time when people may choose self-employment, part-time work or temporary jobs. Dr. Jacquelyn B. James, from Boston College’s Sloan Center on Aging and Work (http://www.bc.edu/research/agingandwork/) calls this “transition” period “the “crown of life”, which implies that it is a special time, perhaps less fraught with the demands of one’s “regular” job which may have consumed years or decades of their lives. According to Wang’s research, “retirees who transition from full-time work into a temporary or part-time job experience fewer major diseases and are able to function better day-to-day than people who stop working altogether.”
At the same time, other research doesn’t focus on the impact of paid work; rather, it notes that as people age, those who stay engaged in life, both socially and intellectually, will fare much better than those who retreat, regardless if they are working for pay or doing something else like volunteering, doing unpaid caregiving work, or just about any activity that engages them.
In my effort to amass retirement narratives, I welcome you to tell me yours! It would be great to hear about your journey, whether you’re in the thinking stage or you have started instituting changes in your paid work schedule, or you have left a paid job and are in a next chapter of your life!
Also, just for fun, check out this video of a policy debate between Republican Paul Ryan who wants to increase the retirement age, claiming that the Social Security fund is depleted, and Democrat Debbie Wasserman Schultz, who strongly disagrees: https://www.youtube.com/watch?v=DIrltAkTf38